by Marie-Léandre Gomez
, 17.04.20
Co-authors:
Marie Kerveillant, PhD ESSEC and ESSEC MBA graduate (E10). Research engineer at ESSEC Business School and Assistant Academic Director of the MGO program at ESSEC Executive Education. Contact: Marie.kerveillant@essec.edu
Matthieu Langlois, Resuscitation anaesthetist, Head of the Dynamo Unit, APHP Pitié Sorbonne Université. Contact: Matthieu.langlois@aphp.fr
Introduction [1]
Under the current crisis conditions, hospitals are facing a massive influx of patients, putting strain on the organization of teams. At the Pitié-Salpêtrière hospital, teams have been working for several years on how to manage extreme crises (terrorist attacks, pandemics, industrial accidents), with tactical medical teams like those of special forces [2]. But how do these teams go from the preparation and organization phase to action, given that putting the plans in action involves many more staff, and how do they adapt practices and recommendations to the specific needs of the current situation? Here, we explain the specificities of high-trust organizations in crisis mode, and explain how the tactical medical teams have built a crisis-mode organization. We will also discuss how the organization has adapted, which was used to inform other Crisis Medical Directors and their offices in other hospitals. Finally, we will provide key takeaways and managerial recommendations for managers dealing with the same crisis.
Organization and coordination of high-reliability organizations in crisis mode
Management research has highlighted the importance of “high-reliability” organizations (HROs), like air traffic controllers, nuclear centres, criminal police services, and hospitals [3]. These organizations are typically the first ones to develop ways of working during a crisis. They operate in an environment with complex, high-risk activities that can potentially lead to major accidents, requiring a high level of security over a long period of time and specific organizational methods to manage in the event of a crisis, with precise coordination and communication processes and decision-making. In the event of a crisis, it is critical that the actors in charge of critical activities have a collective awareness of the situation (collective mindfulness) that permits them to adapt to new, sometimes disruptive, information and share it amongst themselves and that they are able to engage in both individual and collective sensemaking to act in the most effective way possible (enactment). In a word, teams in high-trust organizations prepare themselves for crises, know how to adapt to different levels of crisis, and are prepared to change their mindsets if possible [4]. Their agility during a crisis is the key to overcoming complex and dangerous situations.
The first analyses of the Paris and Oslo terrorist attacks [3] show that it is essential to rethink the empirical and theoretical frameworks we use so that we can better understand the complexity that hospital teams must manage and the way they tend to respond when faced with major crises. In extreme crisis situations, hospitals serve as the cornerstone in managing the flow of sick or injured people. Via its crisis medical director, the hospital has a comprehensive view of the flow of incoming and outgoing patients and can thus develop the best strategy for managing the crisis.
This is the basis of the work on which tactical medical teams and hospital teams have been collaborating for several years now (for example, the collaboration between the Pitié-Salpêtrière hospital and RAID’s tactical medical team): preparing themselves with a cohesive strategy for dealing with unfamiliar situations.
The army, the Army Health Services and interior SWAT teams like RAID have developed the chain of command in operation that has now been adopted by firefighters and inspired the structure of the Crisis Medical Offices in French hospitals. This aims to streamline the flow of information, information processing, writing and analyzing possible situations, and coming up with manoeuvers, with the goal of preserving brainpower for the decision-makers.
When armed forces intervene in a hostage situation, they are operating in an urgent or deteriorating situation. The medical universe in crisis situations is comparable. Moreover, in terrorist attacks where there are attacks at several locations or in the event of natural or industrial catastrophes, all emergency services must act together and in parallel with firefighters, police officers, and hospitals. Coordination should be done with an overall strategy in place, one that does not focus on the influx or the outflux but rather takes both into consideration as well as the onsite capacity. The medical teams must manage process discontinuity, increasing ambiguity surrounding decisions, and mounting interdependence, complexifying coordination within the team and between different teams, to come to a global understanding and avoid silos and division.
Capitalizing on experience and collaborations between tactical medicine and hospitals
Tactical medical teams and hospitals have together faced several crises in recent years, notably for taking care of victims from the 2015 terrorist attacks. Their complementary approaches led them to build an innovative shared methodology.
The operational contributions of tactical medicine: the example of RAID’s medical service
RAID has had medical support for all of its operations since 1994. The doctors who form RAID’s medical service combine regular medical work in emergency rooms or anaesthesia-intensive care with their tactical medicine work with RAID. They also act as coordinators between the traditional hospital world and police services. They are familiar with the functioning of RAID and with the emergency rooms, intensive care units, and surgery departments at their respective hospitals. Tactical doctors dedicate themselves to “rescue and care”, but they are also fully integrated into the assault units. Their mission goes beyond executing technical acts, care, or advice. RAID doctors must also make critical decisions to optimize treatment and evacuation to hospitals. To carry out this mission, doctors must make medical and organizational decisions in highly tactical and threatening situations. Making decisions is common for all emergency doctors, but making them in highly complex and unusual situations is the particular challenge facing the tactical doctors of RAID.
RAID’s teams have shown in recent unprecedented crises that they have impressive know-how enabling them to act and be resilient in difficult and unusual situations, and at the same time coordinate various players who may be less at ease in that type of chaotic environment. Their experience with decision-making when faced with incertitude and management in tactical and operational units may be precious for the hospital teams that must manage the current global Covid-19 pandemic.
The Pitié-Salpêtrière hospital, under the impetus of Professor Riou (then head of the emergency department) understood this challenge after the Paris terrorist attacks, and decided to collaborate with the RAID teams to build a Chief Crisis Medical Office that would make use of the feedback from the decision-making structures of the special forces teams. This collaboration permitted the different players to learn how to work together and to innovate to better manage future crises. In the following section, we present the recommendations from tactical medicine, which have served to organize the Medical Crisis Office in various AP-HP (Assistance Publique - Hôpitaux de Paris) hospitals.
The organization of the Crisis Medicine Office
Since 2016, hospitals must set up a crisis organization structure in addition to their day-to-day organizational systems. During a crisis, hospitals must organize themselves so that they can manage the crisis and work with the first responders. Having an in-house crisis unit enables them to establish a better overall care strategy when faced with an influx of injured or sick people, especially when this influx is spontaneous and due to the hospital in question being the obvious choice of refuge in situations of panic or public health emergencies. The duration and rhythm of the crisis impact the response: after a terrorism attack or industrial accident, the dynamics change quickly. During a pandemic, the situation plays out over a longer period of time. However, the structure and methodology for reacting to the crisis remain the same in both scenarios. Hospitals must nonetheless deal with changing conditions over the course of the crisis, such as the current dwindling stockpile of supplies (materials, antibiotics, anaesthetics) and staff burnout. It is thus of the utmost importance to have a strong system and effective coordination measures so that the organization is able to be flexible and reactive in their decision-making over the crisis and avoid reaching the breaking point.
The organization of a strategic unit of the Medical Chief Crisis Office
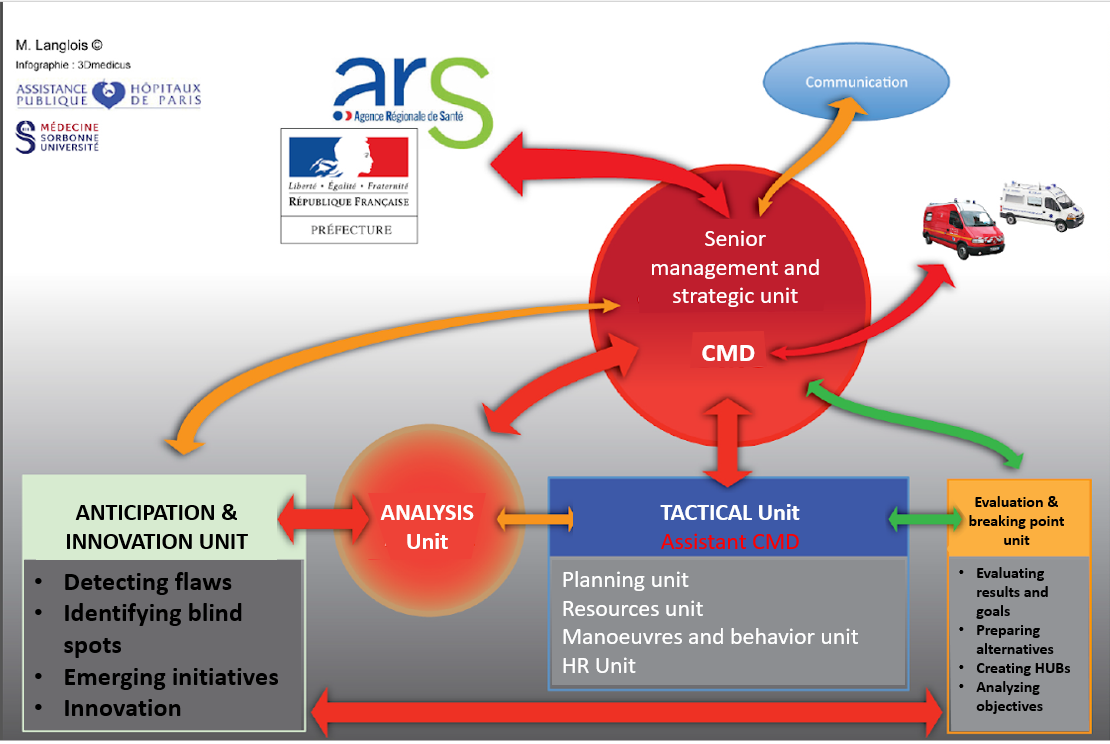
The crisis Medical office is formed of several units, each with their own function. The final decision on strategic matters is made by the Chief Medical Crisis director.
The importance of the Crisis Medical director
The role of the Crisis Medical Director is to help the hospital build a strategy for dealing with unusual situations that still respects standard care procedures. As building such a strategy involves taking risks, the director must be familiar with the type of care given, the hospital’s resources and patients’ prognosis, and have crisis management training. The director cannot wait for a thorough analysis or all possible assessments to begin treatment. As such, the ability to make decisions quickly and anticipe next steps are often essential to guarantee the quality of care.
The crisis medical director has an overall view of the crisis. They are in constant communication with first responders and are familiar with the capacity of their structure, and can organize the flow of patients to maintain an equilibrium vital to keeping the hospital running. The organization of a hospital during a crisis is similar to that of an aeronautical hub. This requires a crisis office that is able to sustain long term analyses and manoeuvres, all the while anticipating and innovating to adapt to the situation.
The role of the crisis medical director is primarily strategic. They create different units that serve to both execute strategic choices and to organize the flow of information to ensure continuity of services, understand unusual situations, and quickly change tactics if necessary.
In critical situations, there must always be equilibrium between a structure that can effectively manage the flow of patients and the quality of care provided. This requires anticipation, agility, imagination, and sometimes innovation.
The strategic unit
This is made up of a small number of people (around 6): a representative of the Crisis Medical Office, a secretary, a coordinator for authorities and institutions, a coordinator for other units, and one or two medical representatives.
The primary role of the tactical unit
The tactical unit, made up of experts in the field, does not concern itself with the overall strategy but rather executes this strategy, identifies primary and secondary goals, and organizes priorities. One of its main goals is to establish a coordination system with the top-level and also cross-department communication. To carry out its missions effectively, the unit must be agile and adaptable, remaining constantly in contact with the evaluation unit. Within the tactical unit, the resources division lists all the resources necessary for effective functioning: beds, medical material, biological material, and logistical tools. It organizes the distribution of these resources based on the predicted length of hospitalization, predicted patient flow, and models that optimize distribution of beds and equipment. The unit works with the evaluation and “breaking point” units to manage the availability of hospital beds and with the innovation unit to come up with new solutions.
The HR unit
The HR unit anticipates staffing needs and acts as a headhunter to recruit for positions identified by the crisis unit. It works in synergy with the resources unit to anticate reinforcement needs and manage the patient flow. The HR unit also arranges for psychological support for the staff.
The innovation unit: where reflection rules
The innovation unit plays a major role, but does not lead the crisis response: rather, its role is reflection. The unit aims to prevent teams from encountering blind spots (such as neglecting non-Covid-19 patients) during their crisis management and by suggesting innovative solutions inspired by feedback from the field and discussions with people in the non-medical world. The innovation unit is not involved with the implementation of solutions. It is linked to the evaluation and analysis units.
The evaluation and breaking point unit
The unit is not directly involved in the hospital’s operations, but its role is nonetheless essential. It analyzes the results and evaluates them relative to the goals and identifies the saturation point, anticipating when it will occur. It raises the alarm when the system is reaching the saturation point. The evaluation unit helps ensure coherence between intermediate objectives and acts as a link between other units.
The analysis unit: eyes on the long-term and normal times
The analysis unit is composed of 5 people maximum: public health researchers, epidemiologists, sociologists, psychologists… It works on a 24/7, permanent basis with the ARS (Autorité Régionale de Santé, the trustee of hospitals). It aims to develop a long-term plan. It is also responsible for recording the crisis and fact-finding, a time-consuming but indispensable activity both for medical and legal reasons and for learning from the crisis.
What are the takeaways?
The crisis puts both hospitals and companies under extreme pressure, requiring a vast amount of resources and staff activity. The way that tactical medicine inspired the crisis management in certain hospitals may inspire both other hospitals and companies to facilitate agility, adaptability, flexibility, and ongoing learning.
A collective organizational crisis response
The first takeaway from tactical medicine is that the crisis responseis organizational: a team effort. The teams prepare for battle in a different way than in their “normal” organization, but there is no room for mavericks or lone heroes. For tactical medicine, decisions are made by the group. All goals must be clear and understood by all so that everyone can adapt their behavior to the new reality. Working in silos, frowned upon in hospitals and in organizations, is no longer appropriate and must be avoided. In hospitals, the evaluation unit can identify the existence of silos.
Structuring the crisis office and its units and assigning roles within small teams is one of the most important parts of the crisis response. The crisis office is organized like a project office and allows for the coordination of actions at all levels by gathering and analyzing internal and external information. It plays a balancing act to maintain perspective over the long term and think of innovative solutions, all the while suggesting concrete actions that will allow senior management to come up with a thorough strategy.
The innovation and evaluation units in some Crisis Medical offices, based on the structure of intervention forces, are a source of inspiration for companies. The innovation unit acts on both a short-term and long-term basis: it makes predictions for the duration of the crisis and after the crisis and also comes up with innovative strategies for the situation at hand.
1. A dynamic plan, not a ballistic one
Many companies have prepared a Business Continuity Plan (BCP) that serves as a benchmark in the crisis. However, seeking to implement the BCP at all costs is not the solution. It is necessary to be able to make it evolve, and to take a dynamic approach to planning, accepting to give up the comfort of a ballistic trajectory provided for in the initial plan, according to the distinction between ballistic and deterministic planning, and dynamic and meaningful planning, analyzed by Philippe Lorino (2019).
Planning is essential because it allows us to anticipate situations, question assumptions, work collectively on courses of action and put ourselves in an analytical position. The arguments of Arie De Geus in "planning as learning" published in 1988 in the Harvard Business Review, are still relevant today. In planning, reasoning, discussions, and brainstorming work count at least as much as the plan itself. You have to know how to deviate from the plan, in a normal situation and even more so in a crisis situation. You must assess the evolution, its means, and government decisions to adapt and innovate. Nothing ever goes as planned. In both normal and crisis situations, organizations can revise their plan while it is being implemented, either to reschedule their trajectory or to replan their objectives. But in a crisis situation, revisions must be more frequent, even daily at present. Actors must constantly ask themselves: what is the current situation? Is the vision I have of it consistent with reality? Are the decisions taken yesterday consistent today? What are the foreseeable situations that await me tomorrow? It is a question of switching to "navigation" mode as opposed to the traditional "steering" mode.
2. Going from steering to navigating
In management, the metaphor of steering has made it possible to highlight the dynamic work of decision-makers, who rely on tools, processes and information systems to act and modify how they act. However, this metaphor often suggests that the pilot's mission is to choose the right roadmap according to the data available to him, from a repertoire of existing plans. However, the experience of tactical medicine in extreme crisis situations seems to us to be more in line with the metaphor of navigation, theorized in strategy by Robert Chia as "strategizing as wayfinding". Sailors try to stay on course and have to deal with environmental conditions that are often too complex and changing too quickly to be modelled before decisions are made, they develop strategies that they re-evaluate very regularly, they use their experience of navigation, their training and their "sense of the sea and navigation", a practical sense, calling on their knowledge as well as their situational awareness.
3. Agile leadership
The management practices of intervention teams such as RAID and tactical medical teams highlight the characteristics of agile leadership in crisis situations. They place themselves in a trial-and-error dynamic, and do not force things: if an action does not work, they try something else. The right to make mistakes is part of experimentation and the search for innovative solutions. Leaders nonetheless require themselves to act quickly and efficiently. Interventions where the situation has deteriorated remind us of the importance of good managers when operating outside the standard framework. The way intervention teams operate also gives us a lesson in humility: leaders take on their responsibilities without seeking merit or recognition, they own their decisions and their consequences vis-à-vis their supervisory authority, the government, and society.
As Dolain, Petitjean and Laborie (2020) note in their recent article on special forces: "Humility and self-sacrifice remain fundamental values. In combat units, there is a lot of emphasis on these qualities: simplicity, good humour, but also a sense of sacrifice for the greater good. This state of mind contributes to the success of the mission. Especially in a crisis situation, you are defeated from the moment you start to think of yourself as a hero, that is to say: alone. Thinking like a champion actually slows down the group, killing its unity, and has indirect effects on the structure, which is the ultimate guarantor of victory. It is also from this humility that the capacity for adaptability comes; it is this humility that protects against the inclination that some people might have to be overly sure of themselves. To face up to it is to leave one's ego aside and to open up to adaptability by refusing to close one's mind".
4. The flow at the heart of the crisis
In hospitals, managing patient flow is one of the main concerns of the Crisis Medical Office. The Crisis Medical Director constantly oversees the flow and reevaluates resources (limited from the start and increasingly scarce), searches for additional resources, and considers the possibility of managing patient flow by organizing transfers. The key reference point is the anticipated breaking point, a threshold that must absolutely not be crossed. All efforts are concentrated on the dynamic between the breaking point and the flow. In businesses, the flow of primary materials or merchandise and monetary flow are a major concern during a crisis. Dynamic management that unites the Crisis Medicine Office can allow a better look at elements that might be coordinated but not necessarily synchronized in real time. Simply sharing information is not enough during a crisis: it is a question of reflecting together to build a global vision, anticipate the effects of decisions as accurately as possible, and therefore increasing sharing information, ideas, and actions.
5. Feedback
Collective learning and sharing experiences are at the heart of crisis management. The Crisis Medical director must also keep in mind that there will be feedback. The goal of this feedback is not to point fingers and identify scapegoats, but rather to learn and understand what lessons can be learned for the reprise of normal activity and to better prepare for future crises. Tactical medical units in SWAT forces go from crisis to crisis, as it is their reason for existing. For most organizations, a crisis is a highly unusual situation. However, a pandemic can also teach us to better prepare for any other crisis that may occur in business, energy, or finance. Moreover, many of the actions experienced during the crisis, and the cross-functional organisations set up, can remain relevant as the situation returns to normal. This feedback must be able to take place quickly and be based on reliable elements. Recording the crisis, as done in the hospital Crisis Medical Office and inspired by the practices of special forces, plays a valuable role in structuring the post-crisis analysis.
Conclusion and takeaways
During this crisis, doctors and other medical professionals are faced with difficult care situations and the disruption of how they normally operate: they are required to function under tense conditions with limited resources. They must face team burnout and resource scarcity. The crisis medicine structure is established to facilitate coordination and decision-making to enable them to work as best they can under stressful conditions. Lessons from tactical medicine and intervention forces are invaluable. There are countless organizations that face these stressors today. As such, we can all learn a few lessons from tactical medicine, namely:
-
Organizing and structuring the crisis response into agile sub-units
-
Using the business continuity plan dynamically (i.e., being flexible and quick to react)
-
Keeping an eye on changes and flow (i.e., patient flow in hospitals)
-
Quickly organizing feedback and sharing information
Footnotes
1. Our work is part of a research project "Crisis organization of medical emergency in the context of disasters", COMED, which is supported and funded by Isite.
2. See the article published on March 20th, 2020 by Dolain, Petitjean & Laborie in Le Grand Continent. [https://legrandcontinent.eu/fr/2020/03/20/faire-face-guerre-coronavirus/
3. As examples of major academic work on the topic, we suggest Weick & Roberts (1993) on air traffic, Journée (2009) and Kerveillant (2017) on nuclear power plants, Schakel et al (2016) on criminal police services, Faraj & Xiao (2006) on hospital emergency services.
4. Lagadec (2020).
5. For information on the 2015 Paris terrorist attacks, see Hirsch et al. (2015) and Service Médical du Raid (2016) and Raux et al. (2019); for information on the Oslo terrorist attacks, Rimstad & Sollid (2015).
References
Chia, R., Holt, R. (2009). Strategy without design. Cambridge University Press.
Dolain, Petitjean et Laborie (2020) : Faire face : 10 points sur la guerre au virus. Le Grand Continent. 20 mars 2020. https://legrandcontinent.eu/fr/2020/03/20/faire-face-guerre-coronavirus/
Faraj, S. Xiao, Y. (2006). Coordination in Fast-Response Organizations. Management Science 52(8): iv-1192.
Hirsch, M., Carli, P., Nizard, R., Riou, B., Baroudjian, B, Baubet, T., et al. (2015). The medical response to multisite terrorist attacks in Paris. The Lancet 386: 2535–2538.
Hunt, P. (2018). Lessons identified from the 2017 Manchester and London terrorism incidents. Part 1: introduction and the prehospital phase. BJM Journal of the Royal Army Medical Corps.
Journé, B.(2001). La prise de décision dans les organisations à haute fiabilité : entre risque d'accident et risque bureaucratique. Cahiers de l'Artemis 3: 101-126.
Kerveillant, M. (2017). The role of the public in the French nuclear sector : The case of "local information commissions" (CLIs) for nuclear activities in the West of France ; Doctoral Thesis, ESSEC Business School.
Lagadec, P. (2020). ): Codiv-19 : L’Hôpital en soins intensifs – Changer de logiciel
https://www.linkedin.com/pulse/codiv-19-lhôpital-en-soins-intensifs-changer-de-logiciellagadec/? published=t publié le 20 mars 2020.
Lorino, P. (2018). Pragmatism and Organization Studies. Oxford: Oxford University Press.
Raux, M., Carli, P., Lapostolle, F., Langlois, M., Yordanov, Y., Féral-Pierssens, A-L., Woloch, A. Ogereau, C., Gayat, E., Attias, A., Pateron, D., Castier, Y., Riouthe, B.(2019). Analysis of the medical response to November 2015 Paris terrorist attacks: resource utilization according to the cause of injury. Intensive Care Medicine 45(9): 1231-1240.
Rimstad, R., Sollid, S. J. (2015). A retrospective observational study of medical incident command and decision-making in the 2011 Oslo bombing. International Journal of Emergency Medicine 8(1), 1–10
Service Médical du Raid (2016). Tactical emergency medicine: lessons from Paris marauding terrorist attack. Critical Care 20(37).
Weick, K. E., Roberts, K. H. (1993). Collective mind in organizations: Heedful interrelating on flight decks. Administrative science quarterly, 38(3): 357-381.